A 49-year-old Romani multigravida woman (history of 8 births) presented to the emergency department of a small district hospital with acute chest pain of 30 min duration and concomitant mild diaphoresis and nausea. Regarding her medical history, she was an active smoker with no other cardiovascular risk factors. Her blood pressure was normal, and her heart rate was 40 bpm. The rest of the physical examination was unremarkable. In the initial electrocardiogram (ECG), ST-segment elevation (STE) was present in leads II, III, aVF, along with ST-segment depression in leads I, AVL and V1-V3. The patient was loaded with aspirin 325 mg and ticagrelor 180 mg. A point-of-care echocardiographic evaluation revealed hypokinesia of the inferior wall, with an estimated left ventricular ejection fraction (LVEF) of 50%. There were no on-site facilities for percutaneous coronary intervention (PCI); thus an emergency transfer was arranged to our primary PCI center, with a transfer time of 30 min. Upon arrival, the patient was subjected to emergency coronary angiography via femoral access, which revealed a normal left coronary system. During contrast injection in the right coronary artery (RCA), a long intraluminal filling defect was demonstrated extending from the ostium to the crux, with compromised flow to the posterior left ventricular artery (PLV) (Figures 1 A, B). Although the coronary angiogram was suggestive of spontaneous coronary artery dissection (SCAD), optical coherence tomography (OCT) was performed to confirm the diagnosis, define the extent of the dissection and guide the potential intervention (Figures 1 C, D). Since the patient remained symptomatic with sustained STE, revascularization with PCI and direct stenting was decided. Unfractionated heparin at a dose of 100 IU/kg was administered intravenously. Finally, five stents were required (Resolute 3/24 mm, 3.5/24 mm, 3.5/24 mm, 3.5/12 mm, 3.5/12 mm) and were implanted from the distal part of the dissected RCA to the ostium in order to achieve full lesion coverage (Figure 2). The angiographic result was satisfactory with subsequent Thrombolysis In Myocardial Infarction (TIMI) flow grade 3 (Figures 3 A, B). OCT was performed, indicating satisfactory stent expansion and apposition (Figure 3 C). The patient was transferred to the coronary care unit, asymptomatic, hemodynamically stable with complete resolution of STE in the ECG. Unfortunately, 90 min later the patient had recurrence of the chest pain along with STE in leads II, III, aVF and V5-6. She was immediately transferred to the catheterization laboratory and emergency coronary angiography through the radial artery was performed, revealing progression of the dissection in the PLV (Figure 4 A). Three more stents were deployed, until full restoration of flow and a good angiographic outcome were achieved (Figures 4 B–E). Review of the OCT run performed during the first procedure revealed a missed small residual dissection at the distal edge of the last stent (Figure 5 A, B). We suppose that this might have been the reason for this early progression of the dissection. Thereafter, the patient had a stable clinical course and was discharged 5 days later with dual antiplatelet therapy (DAPT), including ASA 100 mg qd and ticagrelor 90 mg bid for a year, lisinopril 5 mg qd, metoprolol 25 mg bid, atorvastatin 20 mg qd and lansoprazole 40 mg qd. The predischarge echocardiographic evaluation demonstrated an improvement in LVEF. At 1-year follow-up, she remained uncomplicated.
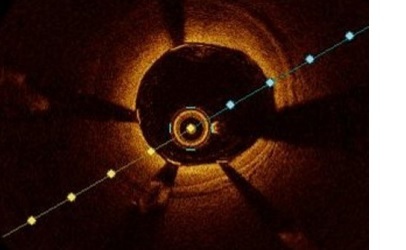
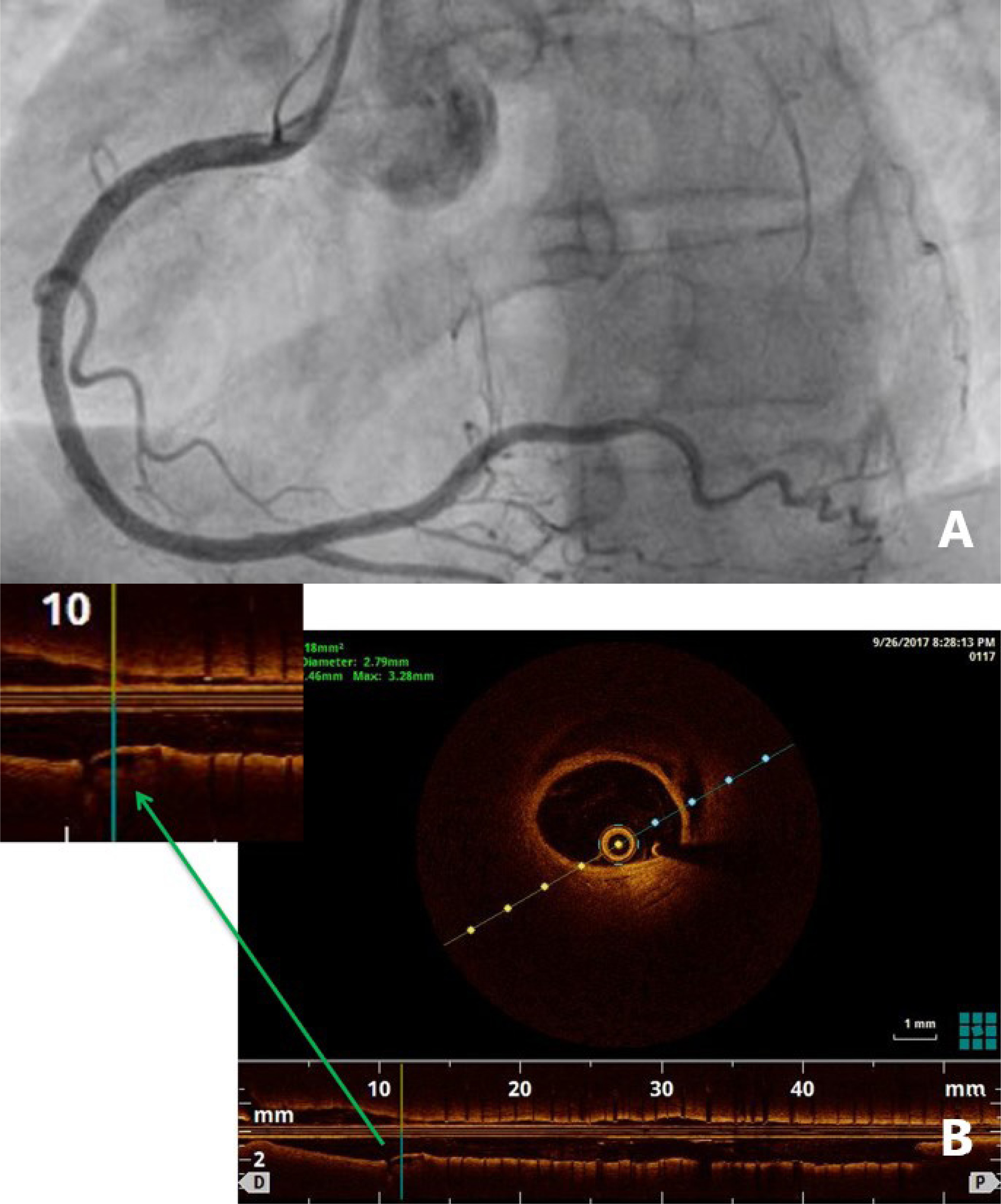
Figure 1
A, B – Right coronary artery with extensive intraluminal filling defect; C, D – optical coherent tomographic run depicting the distal part of the vessel with the 3 normal layers and the distal dissection with the true (TL) and false lumen (FL)
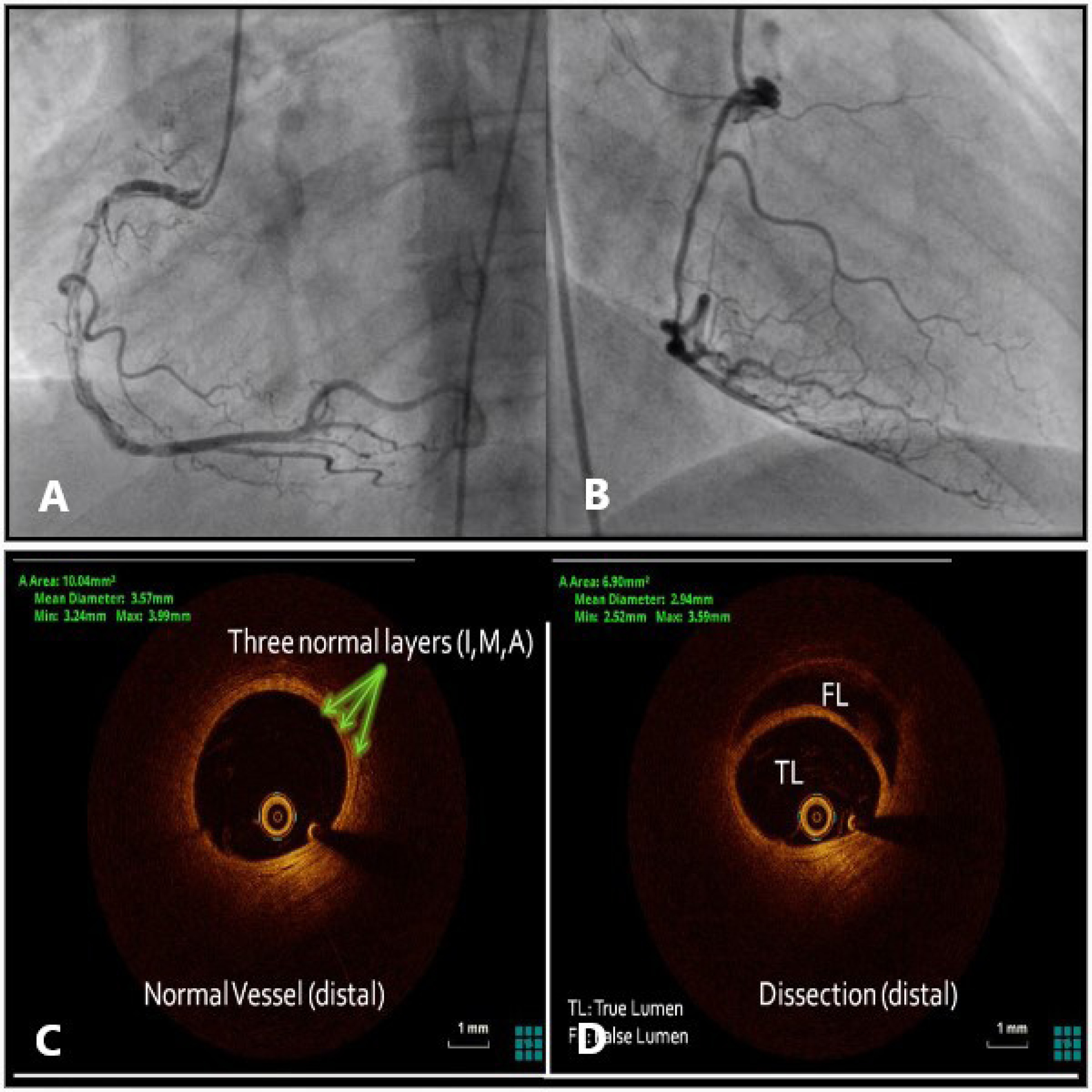
Figure 2
Complex percutaneous coronary intervention of right coronary artery with implantation of 5 stents
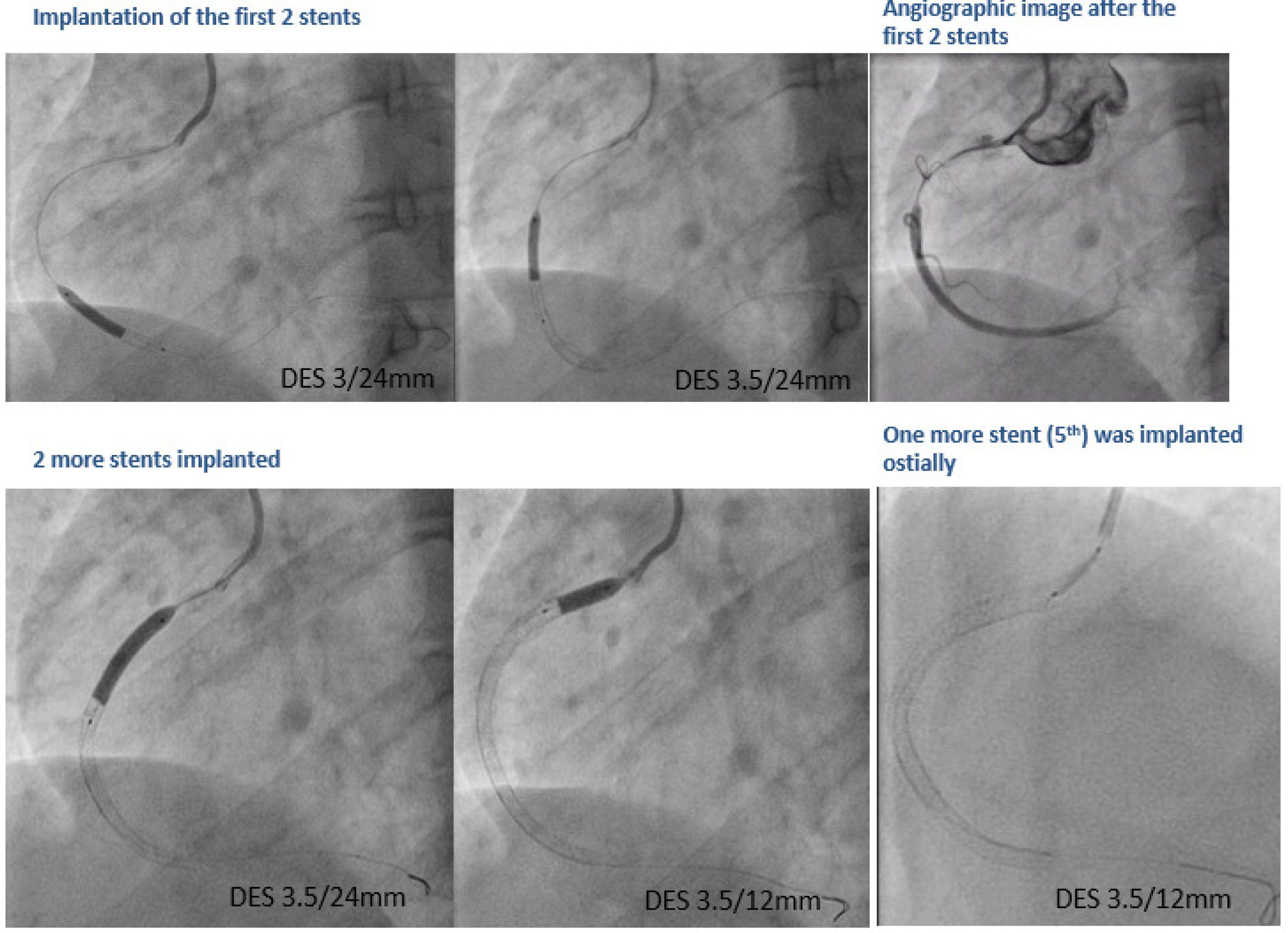
Figure 3
A, B – Final angiographic result; C – Optical coherent tomographic run depicting satisfactory stent expansion and apposition
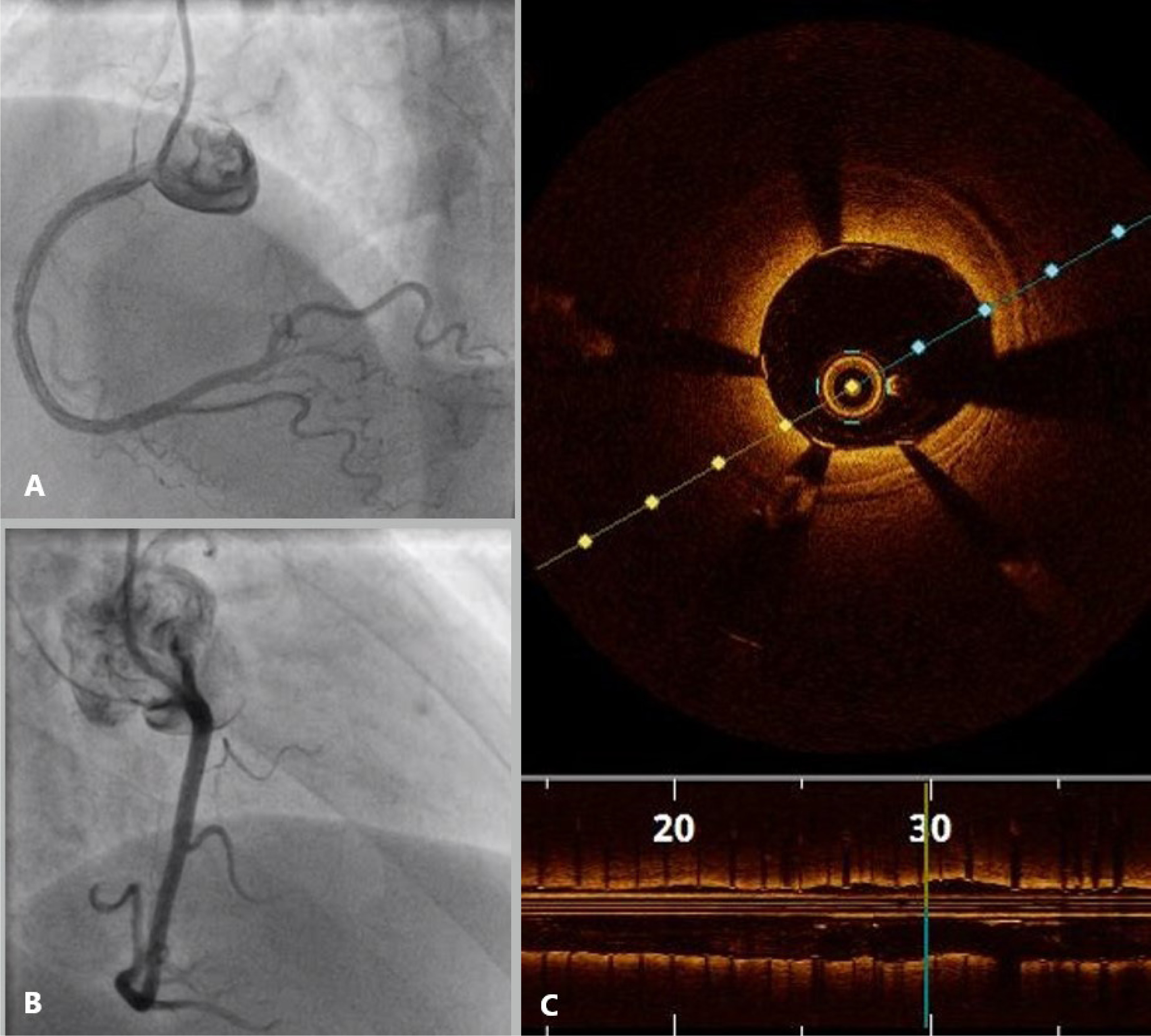
Figure 4
A – Repeat coronary angiography of the right coronary artery (RCA) depicting the progression of the dissection with the compromised flow in posterior left ventricular, B–E – percutaneous coronary intervention in distal RCA with implantation of 3 more stents
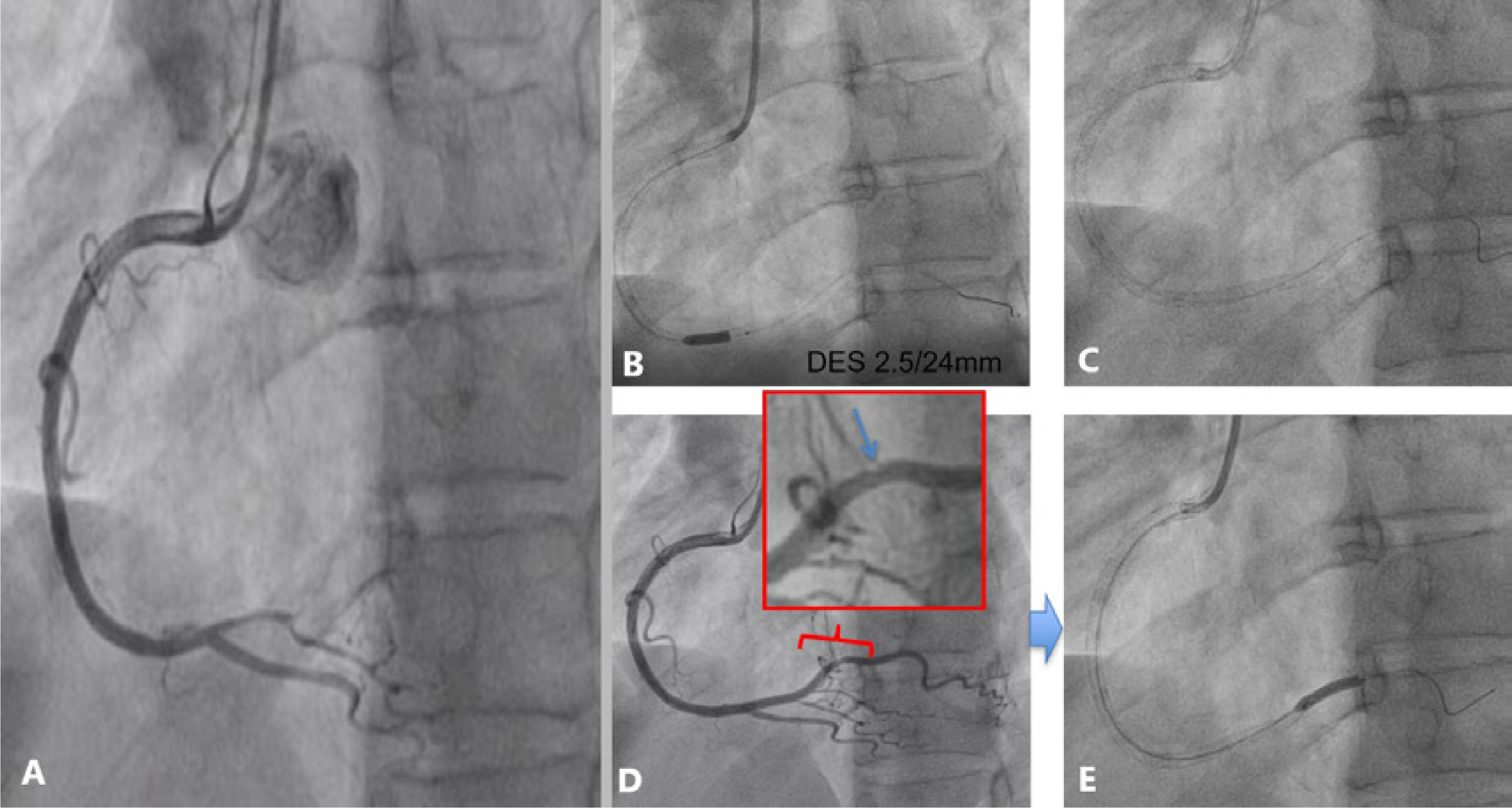
Figure 5
A – Final angiographic result after implantation of 8 stents. B – Optical coherent tomographic run demonstrating the residual dissection at the distal edge of the last positioned stent
SCAD has a predilection for the female gender, accounting for 25–35% of acute coronary syndrome (ACS) in women younger than 50 years of age, implying a potential role of sex hormones in its pathogenesis [1, 2]. It is the most common cause of myocardial infarction during pregnancy and postpartum and constitutes 14.5–43% of pregnancy-associated ACS [3]. The reported relationship between multiparity and SCAD, which is noted in our case as well, may be attributed to the accumulation of changes in the coronary arterial wall mediated by hormonal stimulation during multiple pregnancies, resulting in arterial wall rupture [2, 3]. The mainstay of management in the acute phase of patients with SCAD is the preservation of myocardial perfusion with employment of minimal interventions. The conservative approach, which is the proposed management in the majority of cases, has favorable outcomes, with angiographic indications of healing in up to 70–97% of patients 30 days after the index event [2]. However, an interventional approach was warranted in our case due to the active ischemia, despite the potential complications and the low success rate of PCI in SCAD, reported in about 30% [4]. The high rate of failure is associated with several factors. Firstly, the dissection or the intramural hematoma may extend either antegradely or retrogradely after the stent deployment, as in the case of our patient. The antegrade propagation of the dissection caused distal obstruction of the PLV, which required emergency repeat PCI with subsequent stenting of a substantial vessel segment, increasing the risk of stent thrombosis. Secondly, the advancement of the guidewires, balloons or stents into the false lumen can cause obstruction of the true lumen. Furthermore, even if the PCI is technically optimal during the procedure, gradually the absorption of the hematoma may lead to late stent malapposition, again increasing the risk of stent thrombosis. Emergency repeat PCI has been reported in 4% of SCAD patients initially treated with PCI [2]. The proposed measures to minimize PCI failure in the context of SCAD include the use of cutting balloon angioplasty, direct stenting (as was performed in our patient), proximal and distal edge stenting and bioresorbable scaffolds. Taking into account the challenging nature of PCI in SCAD, the use of intravascular imaging can provide significant information and guide a safer procedure with more favorable outcomes. OCT is superior to intravascular ultrasound (IVUS) in SCAD, due to its higher spatial resolution that allows detailed visualization of the true lumen and any associated thrombus, false lumen dimensions, intramural hematoma extension, the presence of fenestrations or even the intimal tear. IVUS confers a less accurate depiction of the above-mentioned abnormalities, but when available it can help in the diagnosis of SCAD [5]. In general, intracoronary imaging poses risks rising to 8% in SCAD patients including dissection extension with wire placement, guide-catheter iatrogenic dissection, catheter occlusion of the true lumen, and hydraulic propagation of the false lumen during contrast injection in OCT [6]. Thus, it is reserved for cases of uncertain diagnosis or when PCI is decided. In our patient, OCT was used diagnostically and during PCI to confirm that the guidewire was positioned in the true lumen and to estimate the longitudinal extent of the false lumen. The true vessel diameter was also assessed in the proximal and distal edge, in order to prevent late strut malapposition once the hematoma resolved. However, the oversight of the small residual dissection at the distal edge of the last stent (Figure 5) may have triggered the extension of the dissection. Perhaps covering this lesion and 5–10 mm distal to it in healthy borders, as is currently encouraged [2], could have sealed the dissection and might have prevented its progression. Nevertheless, it is possible that the procedure per se could have also led to propagation of the dissection. Even so, interventional cardiologists should be familiar with the optimal use of intracoronary imaging in this specific context in order to achieve more favorable outcomes. SCAD is a well-recognized entity of ACS with a challenging diagnosis and unpredictable course. Although the current practice advocates conservative management, there are cases where revascularization is the only reasonable option. Intracoronary imaging and the implementation of specific PCI strategies may minimize the risk for periprocedural complications in this context.